
30th April 2000
News/Comment|
Editorial/Opinion| Business| Sports|
Sports Plus| Mirror Magazine


Second opinion
Afraid to tread on marbled floors of private hospitals
The Government announced some months ago that it would be enacting new legislation to regulate private health care institutions. Caught in the general turmoil of the country, this new legislation has not been heard of recently and appears to be in limbo.However, we did see new laws being enacted to regulate blood transfusions, explicitly banning such services in the private sector. That was a laudable move, not only because trading in blood is morally and ethically repugnant but also because it represents a serious health hazard in the form of diseases communicable through blood.
Now, private hospitals need regulation. There has been a recent influx of overseas investors promoting private hospitals. Local investors have also taken the plunge, because from all available evidence private hospitals are good business- and often little more than that.
It is not that the concept of private sector health care should be discouraged. In fact, it needs encouragement, for it relieves the burden on the state sector thereby making that sector more accessible to the less affluent. But it does not mean that the private sector in health care should be given a licence to fleece the public with no consideration for ethics, common courtesies and in some cases even minimum standards of care.
Most private hospitals are notorious for exorbitant 'hidden' charges. Drugs given in hospitals are three-to-four- fold more expensive than those available in pharmacies and so are other accessories. Doctors' charges, nursing charges and room charges are not regulated, so patients are at the mercy of the hospital unless they have insurance cover. Patients may be cured of their illness, but they may die of the hospital bill!
Another aspect of this lucrative trade called 'medicine' is the channelled consultation service. Various doctors charge various fees for various lengths of time spent on the patient. There is no regulation whatsoever. Other medical mudalalis use the channelled consultation service for just that- as a channel to obtain a hospital bed and preferential treatment in the state hospital where they are permanently employed.
These are mere statements of fact which are known to the pauper, prince, patient and practitioner alike. It does not take a genius to come to terms with these realities a single visit to a private hospital on a busy working day will suffice. Yet, our health authorities who rush in to admonish doctors' trade unions have feared to tread on the marbled floors of the private hospitals.
The present Minister of Health has often proclaimed he would put an end to all this and bring private hospitals under surveillance. It cannot be difficult. Hotels have a similar scheme: they are rated - with stated minimum facilities for each rating- and their charges are regulated. Hospitals can have a similar scheme.
Surely, charges levied for drugs, investigations and procedures can be regulated too. Other countries have done so with success. And doctors' fees must also be regulated according to the time spent on each patient, so that the prescription is not written as the patient enters the consultation room.
Mere talk of bringing private hospitals under the rein of the Health
Ministry is not sufficient, Mr. Minister. Go ahead and do it and you will
win the eternal gratitude of the long-suffering patient population of this
country and enough votes to win the next election, if that's important
for you!
Bandi paining
By Chris Fernando
Q: I am a 45-year-old housewife with three children. Since of late, I have been suffering from recurring abdominal pains. My family doctor prescribed some medication, which relieved the pains. But I've begun to worry because these pains keep coming back more frequently. I was advised by a friend to see a specialist and get a colonoscopy done. Is this necessary? Do I have anything to worry about?A: Your case certainly needs looking into. Considering that you have been getting these pains on and off, you should not ignore them. Your problem could be due to a number of reasons, harmless or otherwise.
 Let
me give you a general idea of what causes abdominal pain, which is a common
complaint experienced by almost everyone.
Let
me give you a general idea of what causes abdominal pain, which is a common
complaint experienced by almost everyone.
When making a diagnosis, the nature of the pain is a significant factor to a surgeon -whether it is a colicy pain or a constant ache, whether or not it radiates from one area to another. The other important thing is the location of the pain.
It is important to note that any pain can be due to a simple intestinal colic brought on by constipation or indigestion or something worse like a growth in the internal abdominal organs. Therefore, abdominal pain must not be ignored or unchecked.
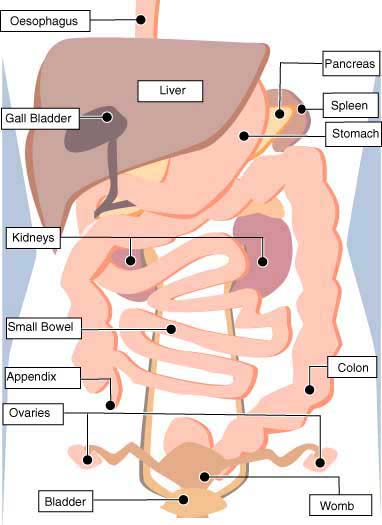
When a patient complains of abdominal pain, a doctor has to check the exact location of the pain, which arises most often from the underlying organs. For e.g. a pain in the right upper abdomen can be due to problems with the liver or gall bladder.
Pain in the upper abdomen above the navel up in the epigastrium can be due to problems with the stomach. Pain arising from the left upper abdomen can be due to problems with the spleen or large bowels. Pain in the middle of the abdomen of colicy nature could be caused by small bowel problems. Pain usually arising from the lower abdomen to the right side can be due to appendicitis, constipation or in a female, problems with the ovaries.
Pain in the left lower abdomen arises from problems in the sigmoid colon, which is the largest part of the large bowel. These can be due to irritable bowels, constipation, diverticulitis, etc. In females, left ovarian problems can cause pain in the left side. Pain arising from the back in the region of the loins is usually due to problems with the kidneys and pain in the upper back can be due to problems with the spinal bones or with an organ known as the pancreas.
It is also important to consider symptoms such as vomiting, diarrhoea, urinary discomfort etc.,that arise with the pain, as they help to point a finger to the affected organ. Abdominal pain associated with discomfort and a burning sensation when passing urine is most likely due to a urinary infection. Pain with vomiting and burning epigastric discomfort can be due to gastritis or gall bladder disease.
Gastritis has now become a fashionable term and people tend to use it for any sort of abdominal pain. But it is very dangerous to diagnose and treat gastritis without a gastroscopy.
I have seen people treating themselves for gastritis when no investigations have been done to diagnose their illness. The danger is that without a gastroscopic diagnosis, one may go on treating some other pain, which arises from the pancreas or the large bowel mistaking it for gastritis, till the situation turns into something more dangerous.
The abdomen itself can be considered a closed bag, which contains the offending organs. The history of the patient will give the doctor an idea of the affected organ, but it is mandatory to perform an X-ray, ultra-sound scan or a CT scan to pinpoint the affected organ. These investigations are freely available and very accurate and specific.
With these investigations, a doctor can accurately pinpoint the affected organs prior to surgery. Gone are the days where operations were done in the hope of finding the affected organ. An ultra sound examination will detect gall bladder disease 100% accurately and can be considered a gold standard for such diseases. Ultra sound and/or the CT Scan can also detect any cysts or growths.
Basically, ultra-sound examinations will reveal problems with solid organs like the liver, kidneys, ovaries and major blood vessels. Further CT scanning will clarify the situation.
However, minor to moderate changes of the inner lining of the stomach, swallowing passage (oesophagus) and the large bowel can only be detected by endoscopy, gastroscopy and colonoscopy. A left-sided abdominal pain in the individual can be caused by a growth in the large bowel which could be confined only to the inner lining. An ultra sound or CT Scan will not reveal anything. However, a colonoscopy will diagnose the illness immediately.
Recently, I performed emergency abdominal surgery on a patient for obstruction of the bowels. In the past year he had been having abdominal discomfort and pain with constipation, on and off. The X-rays and ultra-sound examinations had been performed elsewhere, but all these were found to be normal. No one had bothered to do a colonoscopy.
By the time he came in for surgery, his bowel was completely blocked with an advanced growth in the colon, which could easily have been detected an year ago at the onset of his symptoms, if a colonoscopy had been done.
This example emphasises the fact that some abdominal pains due to growths such as these which arise from the inner lining of the intestinal tract can only be detected by endoscopic procedure such as colonoscopy of the large bowels and gastroscopy of the stomach and swallowing passage. It is only a colonoscopy, which is an endoscopic procedure done under mild sedation that will detect the growth.
It is of vital importance for abdominal pain to be correctly localised to the anatomical organ, which it arises from and further tests such as an X-ray, ultra- sound, CT Scans and endoscopy undertaken to detect pathology.
Blood investigations are also performed to detect abnormalities of the internal abdominal organs. Liver disease can be detected by abnormalities found in the liver function test.
Pancreatic abnormalities can be detected by blood tests and also by ultra- sound examinations. A simple urine test will reveal a fair amount of bladder and kidney pathology but this will have to be coupled with renal function tests.
Furthermore, most internal abdominal organs such as the liver, gall bladder, stomach, intestines, womb, ovaries and the inside of the abdominal cavity can be seen as they are by laparoscopy, which is a procedure done by introducing a small camera, which is slightly bigger than a pen, via a very tiny incision in the abdomen. By these tests, abdominal pain can be localised to the offending organ and treated adequately.
No abdominal pain, however slight, should be ignored and treated lightly. I would advise you to get your illness further investigated to arrive at a definite diagnosis.
Dr. Maiya Gunasekera, MBBS Hon (Cey.) M.S. FRCS (Eng) FRCS (Ed) FICS
Fellow Sri Lanka C.S, is Consultant Surgeon/Gastro Enterologist at the
Nawaloka Hospital.
Breast is best for baby
Working mothers are becoming increasingly common in Sri Lanka. After childbirth, they are granted 84 working days of maternity leave, but most of them are still breast-feeding their babies when they return to work.Weaning foods have to be introduced when the baby is four months old but most mothers want to continue breast-feeding and indeed they can do so, provided they do not have to return to work. There is a solution to this problem expressing breast milk, storing it suitably and then feeding it to the child later. This way, the child continues to get breast-milk and the mother can return to work.
Feeding Expressed Breast Milk (EBM) is widely practised in developed countries and is being encouraged in Sri Lanka. Here are a few hints on how to do it:
* Wash hands thoroughly before expressing milk.
* Prepare a container for EBM- a cup, glass or jug with a wide mouth. Wash it in soap and water and then pour boiling water into the container and leave it for a few minutes. Pour the water away, just before expressing the milk.
* Expression of milk from the breast can be done standing or seated, but the mother must be comfortable. Milk is expressed, using the thumb and index finger.
* Express one breast for two to four minutes until the flow slows; then express the other side. Repeat both sides alternatively until the milk stops flowing.
* It takes about half an hour for sufficient milk to be expressed, so this cannot be done in a hurry, when the mother is just about to go for work and is running late.
* The milk should be stored with the container closed- to prevent entry
of other substances - in the refrigerator in the non-freezer compartment.
Hepatitis B-the silent killer
Hepatitis B is increasingly being recognized as a common but under-diagnosed viral disease with potentially fatal consequences. An estimated 2000 million - 40% of the world's population - is thought to be infected with the virus and about a million people die from the disease every year. Yet, the disease is preventable to a large extent.Hepatitis is inflammation of the liver and the most common cause is infection with one of five viruses called Hepatitis A, B, C, D and E. All these viruses can cause sudden symptoms including yellowing of the skin and eyes (jaundice), dark urine, nausea and vomiting and abdominal pain.
However, some of these viruses can cause a chronic carrier state in which the patient never gets rid of the virus and may later develop cirrhosis of the liver or liver cancer.
Hepatitis B is a virus of this type and is the most serious of viral hepatitis. It is transmitted by blood and sexual contact, very much like AIDS - but it is 50 to 100-fold more infectious than AIDS. It is also transmitted to newborn babies if the mother is infected. It can also be transmitted through injections using unsterilized needles. For this reason Hepatitis B is an occupational hazard for health workers. Unlike some other forms of hepatitis, Hepatitis B is not transmitted by contaminated food or water. It is also not spread by casual contact.
Because of poor screening facilities for blood products hepatitis has become common in developing countries. In Africa, about 10 per cent of the population carries the virus.
In the Indian subcontinent and the Middle East, about five per cent of the population is affected. In Western Europe and North America, the rate is less than one per cent. No precise data are available for Sri Lanka.
The disease is prevented by a vaccine, which has been used extensively since 1982. The vaccine is 95% effective in preventing children and adults from becoming carriers of the virus if they have not yet been infected. Even if infected, the occurrence of liver cancer declines dramatically in immunized children. In that sense, this is the first vaccine developed against a cancer.
In Sri Lanka now, workers in the health sector are routinely administered the vaccine at regular intervals. The vaccine is also available to the general public on prescription.
Liver cancer the most feared outcome of Hepatitis B, is usually fatal and unfortunately develops between the ages of 35 and 65 when people are maximally productive and trying to raise their children. Treatment earlier consisted of chemotherapy which only prolonged the life span by a few years.
Now the disease is treated with a new drug, 'Interferon' which is more promising. Yet, this drug is very expensive even in developed countries and will not be available on a regular basis in Sri Lanka in the near future.
The newest option in treatment is a liver transplant which has been attempted successfully in many western countries.
Considering these factors, it is only prudent that populations are screened
and vaccinated against Hepatitis B. The World Health Organisation has called
for the Hepatitis B vaccine to be included in national immunisation programmes
and about 100 countries have done so.
Big ban
Recently, much was made of the decision by Sri Lanka's monopoly tobacco manufacturer to stop all forms of advertising.Even though belated, this is a move in the right direction.
Nevertheless, there is more the government can do to reduce the smoking habit in the country and thereby save valuable funds spent treating smoking related diseases.
Countries such as New Zealand and Thailand which recently introduced comprehensive tobacco control policies have reported a ten per cent drop in tobacco sales after the new regulations were enacted.
This is what the World Health Organisation recommends to governments to create a comprehensive tobacco control programme:
* Ban all tobacco advertising and promotion.
* Ban sale of cigarettes to children.
* Have mandatory health warnings on all tobacco products.
* Protect people from involuntary exposure to tobacco by establishing smoke-free public places.
* Bring tobacco smuggling under effective control.
* Regulate and regularly increase the price of cigarettes.
* Use part of the revenue from tobacco taxes to promote health care.
* Invest in tobacco related health education.
* Invest in providing facilities for rehabilitation of tobacco users.
* Encourage media involvement in tobacco control.
Tobacco abuse is after all, a serious health problem: Illnesses attributable
to tobacco smoking kill four million people every year or one every eight
seconds.
Diabetes: it's getting younger
Earlier, the profile of a diabetic was that of a middle-aged person, often well into his forties. Though younger diabetics- even children- were well known, researchers are discovering a new trend the age of detecting diabetics is lower and the disease is increasingly being diagnosed in younger people.The incidence of diabetes has anyway been rising, due partly to greater awareness of the disease among the public, leading to more frequent testing and detection.
But now, a trend is seen where people younger than 40 are prone to the disease: in Hong Kong in 1999, 28% diagnosed with diabetes were in their thirties or younger. A similar picture is emerging in Singapore.
Researchers believe the trend could be due to an aggravation of risk factors in the young- over-indulgence in rich food, little physical activity and also stress.
The problem lies in the fact that the younger you are the more vulnerable
you will be in developing complications of the illness, which could be
serious eye, kidney and nerve damage.
AIDS what's new?
Research is progressing at a hectic pace to find a cure for the scourge of our times, the Acquired Immune Deficiency Syndrome (AIDS).What is the state of the research field right now and is there a cure in sight? What are the latest drugs available?
There has been a spate of anti-retroviral drugs being developed recently. They include three types of drugs: Nucleoside reverse transcriptase inhibitors, non-nucleoside reverse transcriptase inhibitors and protease inhibitors.
In all, there about ten drugs approved for use against AIDS.
Do the new drugs work?
The drugs are used in combination with each other and different combinations are being tried out. While there have been no reports of a 'cure', the combined use of these drugs has led to a decline in AIDS-related deaths over the past year.
The efficacy of combination therapy has also been demonstrated in asymptomatic persons who carry the infection- the amount of the virus in the blood falls to an almost undetectable level. It is still not known, however, whether the drugs can eradicate the virus from the nervous system or whether a reduction in the virus level leads to prevention of transmission of the illness to others.
How expensive is the new treatment?
Again, they are very expensive, costing about US$ 1000-1500 a month. Therefore they are beyond the reach of governments in the developing world where 90 per cent of all HIV-infected persons live. Sri Lanka at present has no policy of supporting expensive AIDS therapy in the government sector.
Are these drugs available in Sri Lanka?
While the newer anti-AIDS drugs are not available, the 'older' anti-AIDS drugs can be ordered in the private sector, though the cost is prohibitive.
Treatment of the few dozen AIDS patients in this country is mostly supportive, treating the infections and other complications that they may be suffering from.








![]()
Front Page| News/Comment| Editorial/Opinion| Plus| Business| Sports| Sports Plus| Mirror Magazine
Please send your comments and suggestions on this web site to